Tuesday, June 16, 2020

The 161-page proposal, officially posted Monday in the Federal Register, would also streamline the asylum-approval process, letting immigration judges rather than immigration courts make rulings in asylum cases and redefining the definition of a frivolous application.
The proposal follows similar actions by the departments of Homeland Security and Justice, but legal experts say this time it will be harder to challenge in court than those previous rules.
“Essentially this rule tries, in a way that hasn’t been done before, to define what can be grounds for asylum,” said Jessica Bolter, an associate policy analyst at the Migration Policy Institute.
The proposal, first unveiled Wednesday, was swiftly condemned by advocates like the Tahirih Justice Center, which called the proposed regulations “an assault on the fundamental right to seek asylum.”

The Arizona-Sonora Desert Museum began a phased reopening today, June 16, with new safety precautions based on the Center for Disease Control and Prevention guidelines.
The natural history museum, located at 2021 N. Kinney Road, is also a zoo, botanical garden, and aquarium. Before the COVID-19 outbreak, they frequently hosted art gallery events and educational programs for children and adults of all ages.
Guests who plan a visit to the museum will still have access to most exhibits. Some indoor amenities will be closed, such as the Packrat Playhouse, while others will be modified to ensure health safety. Food and beverages will still be available onsite.
Tags: COVID-19 , Coronavirus , Arizona-Sonora Desert Museum , Reopen , Safety , Social Distancing , Image
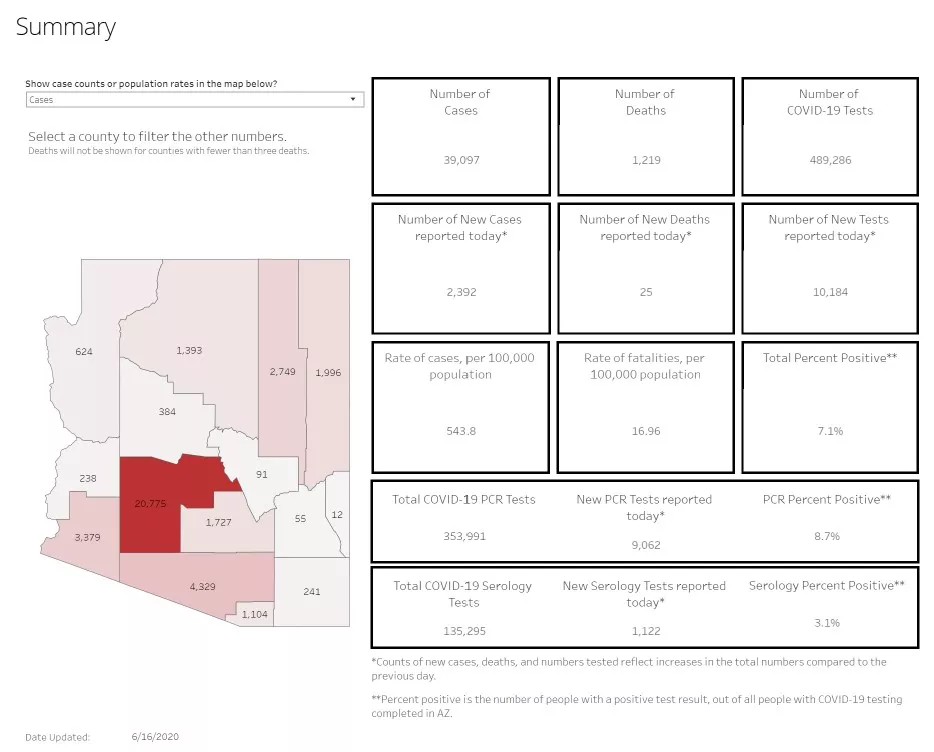
Pima County had 4,329 of the state's 39,097 confirmed cases.
On June 1, the state had 20,123 confirmed cases.
A total of 1,219 people have died after contracting the virus.
Maricopa County has more than half the state's cases, with the number of confirmed COVID-19 cases hitting 20,775.
Because symptoms can take as long as two weeks to appear after exposure to the virus (while some people can remain entirely asymptomatic), health officials continue to urge the public to avoid unnecessary trips and gatherings of more than 10 people, especially if you have underlying health conditions, and have advised people to cover their faces with masks in public.
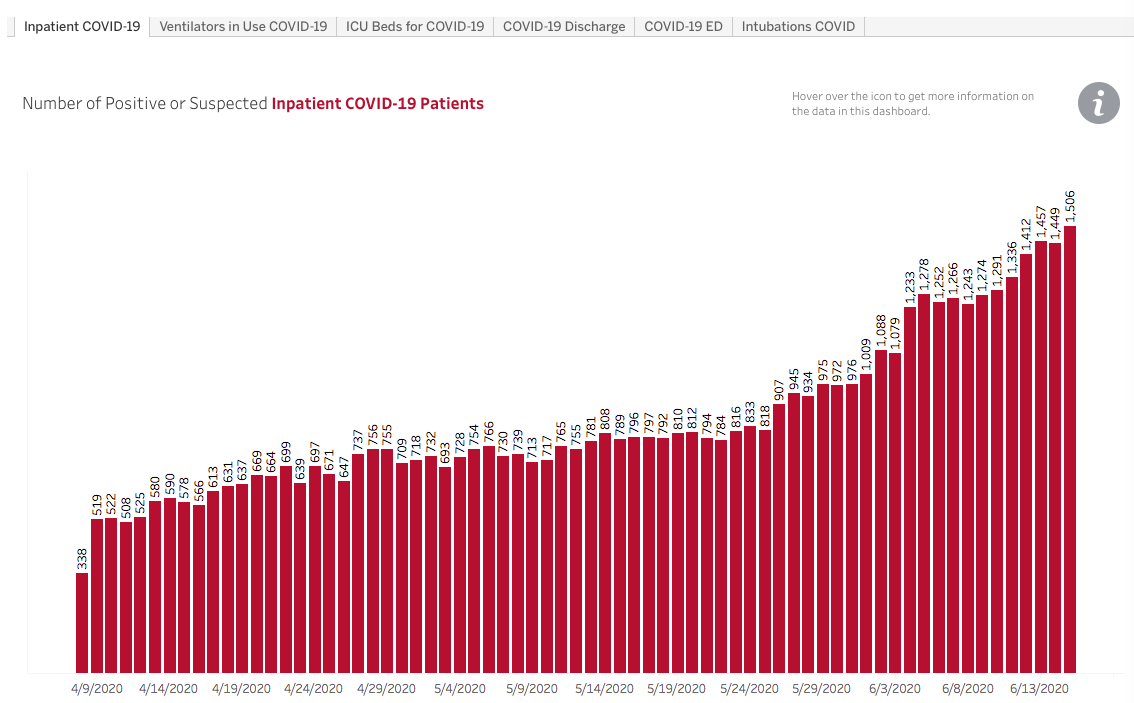
Although Gov. Doug Ducey told Arizonans that the state "was clearly on the other side of this pandemic" when he lifted his stay-at-home order on in mid-May, Arizona hospitals continue to see a steady rise in the number of people hospitalized with COVID symptoms, as well as more people visiting emergency rooms.
This morning's Arizona Department of Health Services report shows that as of yesterday, a record 1,506 Arizonans were hospitalized, a jump of 497 from June 1. A record number total of 956 people arrived at emergency rooms with COVID-like symptoms on June 15, according to the report. Previous to June, the number of people seeking help in emergency rooms never topped 667, but the daily number hasn't dipped below 800 since June 5. The number of patients in ICU beds hit a new record of 502 yesterday.
Tucson officials, including Mayor Regina Romero and Tucson City Councilman Steve Kozachik, have asked Ducey to allow local communities to set their own standards to reduce the rapid spread of COVID-19. Under his executive order, Ducey has prohibited local jurisdictions from setting standards tougher than state regulations.
Romero yesterday urged Ducey "to remove the restrictions he has placed on local governments from taking their own public health measures."
"For example, I believe that face masks should be mandatory in areas of the state with high community transmission for indoor spaces where social distancing is not feasible," Romero said. "Gov. Ducey needs to untie the hands of local governments and allow us to make decisions that are in the best interest of our communities and account for local conditions."
Ducey, who has rarely been seen with a mask or face covering and whose administration has frequently neglected to include the advice in various health advisories it has sent out, said last week he did wear them while shopping when he cannot physically distance from others by at least 6 feet. He advised Arizonans to wear them if they felt comfortable doing so.
Despite the rising number of hospitalizations, Gov. Doug Ducey said last week there's no reason to be concerned about hospital capacity.
Monday, June 15, 2020
- The number of confirmed coronavirus cases in Arizona jumped past 36,000 as of Monday, June 15, with a jump of 1,014 new cases reported this morning, according to the Arizona Department of Health Services.
- The Bighorn Fire is now approximately 14,600 acres and is 22 percent contained.
- For weeks, Rachel Willard, the county health director in Wilkesboro, North Carolina, had watched with alarm as COVID-19 cases rolled in from the Tyson Foods chicken plant in the center of town.
- In late March, as the number of COVID-19 cases was growing exponentially in the state, Cuomo said New York hospitals might need twice as many beds as they normally have.
- Two weeks after the polls closed in this year’s Ohio primary, two U.S. Postal Service employees showed up in the office of Diane Noonan, the director of elections in Butler County. The workers carried a tray of 317 unopened ballots that had been sitting in a Postal Service warehouse since the day before the election.
- Escape the summer heat (and quarantine) with the rocking sound of live music, happening every week at The Gaslight Music Hall in Oro Valley. Dance with your friends, enjoy some tunes, and snack on the region’s best pizza.
- Customs and Border Protection officials spent funds that were supposed to go to medical care and migrant processing facilities to pay for computer upgrades, canine units, ATVs and other items instead, a new government report shows.
- If you have kids, summer in Arizona usually contains many trips to the pool, splash pads, museums, or summer camp. This year has been a bit different.
- Sundt Construction Co. and its partner Kiewit picked up an award for their joint efforts on the Ina Road Traffic Interchange earlier this month, the companies announced in a press release.
- Local financial firm Hughes Federal Credit Union recently earned awards for its website, inclusivity initiatives and marketing strategies by Progress Software and the Credit Union National Association, the company announced Monday.
- The University of Arizona will now offer a Master of Arts in Bilingual Journalism, which is expected to prepare future journalists to “cover complex issues affecting Latinx people in the U.S. and abroad,” according to a press release from the UA’s School of Journalism.

The prediction from New York Gov. Andrew Cuomo was grim.
In late March, as the number of COVID-19 cases was growing exponentially in the state, Cuomo said New York hospitals might need twice as many beds as they normally have. Otherwise there could be no space to treat patients seriously ill with the new coronavirus.
“We have 53,000 hospital beds available,” Cuomo, a Democrat, said at a briefing on March 22. “Right now, the curve suggests we could need 110,000 hospital beds, and that is an obvious problem and that’s what we’re dealing with.”
ProPublica is a nonprofit newsroom that investigates abuses of power. Click here to read their biggest stories as soon as they’re published.
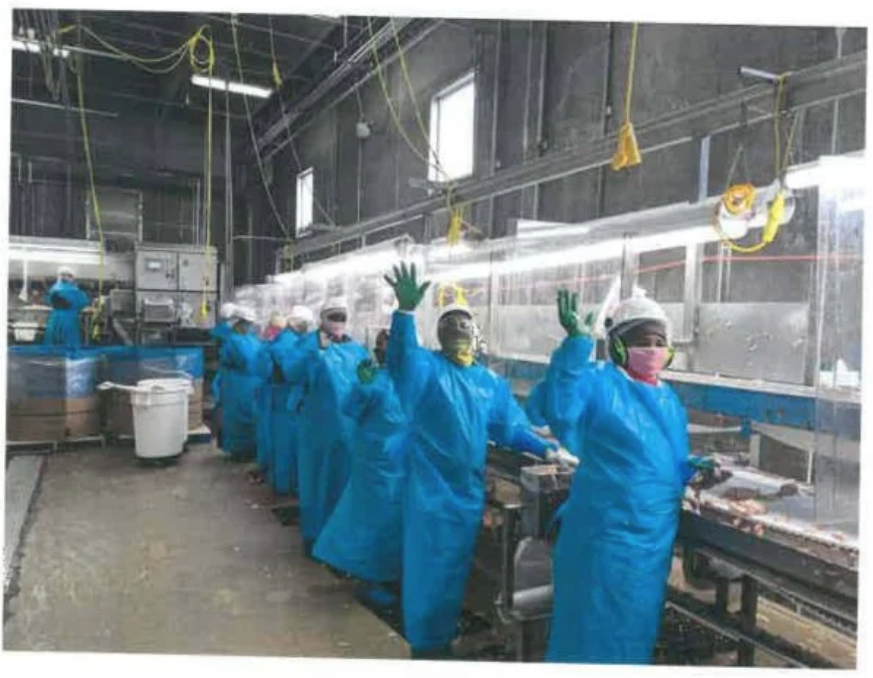
For weeks, Rachel Willard, the county health director in Wilkesboro, North Carolina, had watched with alarm as COVID-19 cases rolled in from the Tyson Foods chicken plant in the center of town. Then Tyson hired a private company to take over testing, and the information suddenly slowed to a trickle.
Blinded to the burgeoning health crisis, Willard and her small staff grew increasingly agitated. The outbreak had already spread across 100 miles of the North Carolina piedmont, and two workers had died. But nearly a week after Tyson’s testing ended in May, the county health agency had received less than 20% of the results. The little information it did receive was missing phone numbers and other data, hindering critical efforts to follow up with infected workers, to tell them to isolate and to trace their contacts.
“Our fear and alarm is the fact that close contacts and positive cases are walking around, potentially shedding the virus and infecting others,” Willard, who was coordinating the response while on maternity leave, wrote to state officials on May 14.
Saturday, June 13, 2020
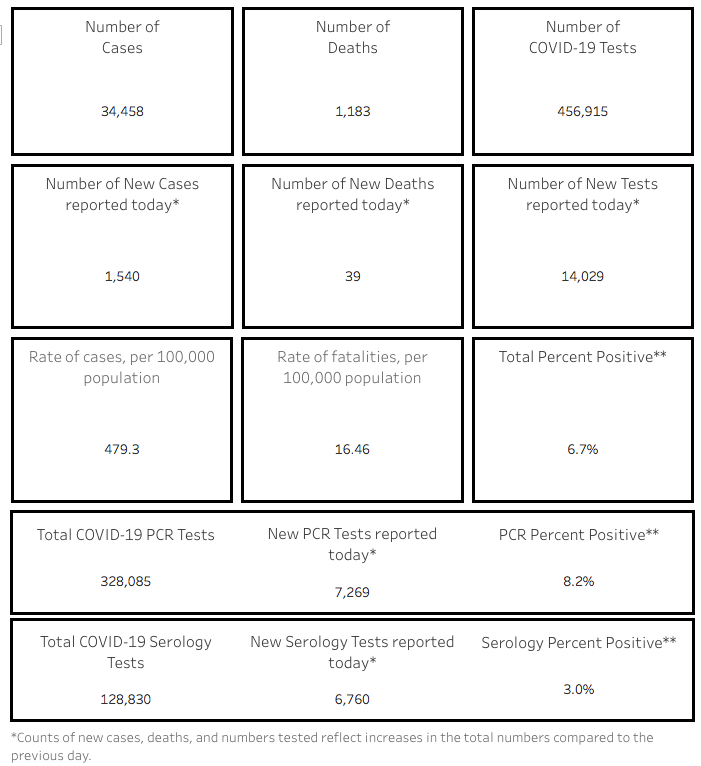
The number of confirmed coronavirus cases in Arizona jumped past 34,000 as of Saturday, June 13, with a jump of 1,540 new cases reported this morning, according to the Arizona Department of Health Services.
Pima County, which saw 261 new cases reported this morning, had 3,889 of the state's 34,458 confirmed cases.
A total of 1,144 people have died after contracting the virus, including 223 in Pima County.
In Maricopa County, the number of confirmed COVID-19 cases hit 17,791.
Because symptoms can take as long as two weeks to appear after exposure to the virus (while some people can remain entirely asymptomatic), health officials continue to urge the public to avoid unnecessary trips and gatherings of more than 10 people, especially if you have underlying health conditions, and have advised people to cover their faces with masks in public.
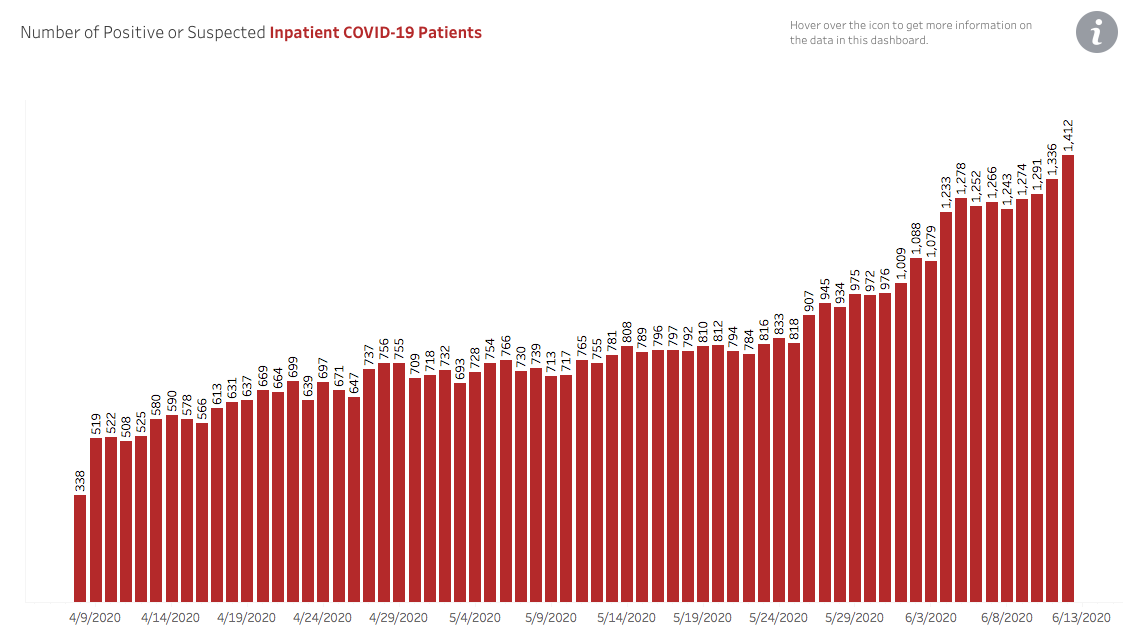
Although Gov. Doug Ducey told Arizonans that the state "was clearly on the other side of this pandemic" when he lifted his stay-at-home order on in mid-May, Arizona hospitals continue to see a rise in the number of people hospitalized with COVID symptoms, as well as more people visiting emergency rooms. This morning's Arizona Department of Health Services report shows that as of yesterday, a record 1,412 Arizonans were hospitalized, a jump of 403 (or 28 percent) from June 1.
For the second day in a row, more than 900 people arrived at emergency rooms with COVID-like symptoms on June 13, according to the report. Previous to June, the number of people seeking help in emergency rooms never topped 667, but the daily number hasn't dipped below 800 since June 5. A record number of 447 Arizonans were in ICU units.
Despite the rising number of hospitalizations, Gov. Doug Ducey said earlier this week there's no reason to be concerned about hospital capacity.
Along with growing cases and increasing hospitalizations, Arizona is trending in the wrong direction in one of the CDC gating criteria that Ducey used to justify lifting the stay-at-home order on May 16. Ducey then noted that CDC gating criteria included two weeks of falling cases or two weeks decreasing positive cases as a percentage of total tests. Total cases continue to rise, as does the number of positive cases as a percentage of total tests. On May 17, the percentage of positive tests to total tests was 6 percent; on May 24, it was 9 percent; on May 31, it was 12 percent, according to figure on the ADHS website.
In a contentious June 11 conference, Ducey acknowledged that trend was moving in the wrong direction and promised the state would continue to monitor that number. But he said the idea of enacting a new stay-at-home order was not under discussion by his administration.
Ducey pushed back at local and national media reports that suggested that the rising cases, increased hospitalization and reversal of CDC gating criteria trends meant that Arizona was moving in the wrong direction. He called reports that the healthcare system was nearing capacity as "misinformation."
He said Arizonans would have to learn to live with the virus.
"This virus is not going away," Ducey said. "There is not a cure for this virus. There is not a vaccine for this virus. So this virus is something we need to learn to live with. And we need to make sure we are protecting the most vulnerable in our society. Those are folks in a certain age bracket with underlying health conditions and at-risk conditions and we're going to continue to do that every single day until there is a vaccine."
Friday, June 12, 2020
Beginning Tuesday, June 16, through Thursday, June 18, COVID-19 antibody testing will be initiated for correctional staff of the Arizona State Prison Complex in Florence through an onsite testing process.
Sonora Quest Laboratories will conduct the tests, which take about 5 to 10 minutes. According to a department press release, these tests are intended to help identify which people have been exposed to the COVID-19 and developed antibodies to fight it.
“This is an exceptional opportunity for the department to provide COVID-19 testing to our brave frontline men and women who continue to serve the public as first responders throughout the pandemic,” said Arizona Corrections Director David Shinn in a press release.
This new development is part of a larger effort within the state government to provide antibody testing for all state prison employees. Back in mid-May, Arizona Gov. Doug Ducey announced plans to prioritize correctional staff for receiving antibody testing. The effort consists of a partnership between the Arizona Department of Health Services and private sector laboratories.
While efforts to test employees is ramping up, testing for people incarcerated in these prisons remains minimal. The most recent data shows just over 2,000 incarcerated people have been tested for COVID-19, with about 1,700 negative results. Just over 250 incarcerated people have tested positive, 130 tests are still pending and 110 people have reportedly recovered from the disease.
There are over 40,000 people incarcerated in state prison facilities.
In addition, 117 staff members have self-reported as positive for COVID-19, with 85 of them reported successful recovery.
Tags: Coronavirus , COVID-19 , Antibody Testing , David Shin , Arizona Department of Corrections , Governor Doug Ducey , Image

In 2017, TeamHealth, the nation’s largest staffing firm for ER doctors, sued a small insurance company in Texas over a few million dollars of disputed bills.
Over 2 1/2 years of litigation, the case has provided a rare look inside TeamHealth’s own operations at a time when the company, owned by private-equity giant Blackstone, is under scrutiny for soaking patients with surprise medical bills and cutting doctors’ pay amid the coronavirus pandemic.
Hundreds of pages of tax returns, depositions and other filings in state court in Houston show how TeamHealth marks up medical bills in order to boost profits for investors. (Some of the court records were marked confidential but were available for download on the public docket; they were subsequently sealed.)
TeamHealth declined to provide an interview with any of its executives. In a statement for this story, the company says it’s fighting for doctors against insurance companies that are trying to underpay: “We work hard to negotiate with insurance companies on behalf of patients even as they unilaterally cancel contracts and attempt to drive physician compensation downward.”
But the Texas court records contradict TeamHealth’s claims that the point of its aggressive pricing is to protect doctors’ pay. In fact, none of the additional money that TeamHealth wrings out of a bill goes back to the doctor who treated the patient.
Instead, the court records show, all the profit goes to TeamHealth.
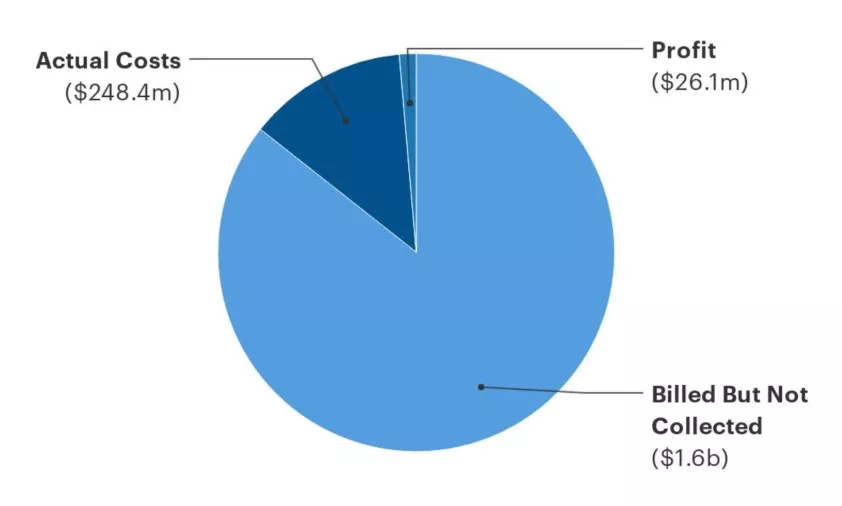
Anatomy of an ER Bill
Two TeamHealth affiliates in Texas billed 7.7 times more than their actual costs of paying for clinicians and support services. The bulk of the charges were discounted or written off. About 10% of the money actually collected went to corporate profits.
“These companies put a white coat on and cloak themselves in the goodwill we rightly have toward medical professionals, but in practice, they behave like almost any other private equity-backed firm: Their desire is to make profit,” said Zack Cooper, a Yale professor of health policy and economics who has researched TeamHealth’s billing practices and isn’t involved in the Texas lawsuit.
“In the market for emergency medicine, where patients can’t choose where they go in advance of care, there’s a real opportunity to take advantage of patients, and I think we’re seeing that that’s almost precisely what TeamHealth is doing, and it’s wildly lucrative for the firm itself and its private equity investors.”
Some of TeamHealth’s own physicians say they’re uncomfortable with the company’s business practices.
“As an emergency medicine physician, I have absolutely no idea to whom or how much is billed in my name. I have no idea what is collected in my name,” said a doctor working for TeamHealth who isn’t involved in the Texas lawsuit and spoke to ProPublica on the condition of anonymity because the company prohibits its doctors from speaking publicly without permission.
“This is not what I signed up for and this isn’t what most other ER docs signed up for. I went into medicine to lessen suffering, but as I understand more clearly my role as an employee of TeamHealth, I realize that I’m unintentionally worsening some patients’ suffering.”
Most ER doctors aren’t employees of the hospital where they work. Historically they belonged to doctors’ practice groups. In recent years, wealthy private investors have bought out those practice groups and consolidated them into massive nationwide staffing firms like TeamHealth and its largest competitor, KKR-owned Envision Healthcare.
These takeovers have affected patients, too, because the groups have gotten into payment disputes with their insurers. As a result, patients can receive huge medical bills even when they pick a hospital within their insurance plan’s network, because the individual doctor working for a contractor like TeamHealth could be out of network. This practice, known as surprise billing, caught the attention of lawmakers who have spent months working on legislation.
TeamHealth said surprise bills are “rare and unintended,” but with millions of patients, it has happened tens of thousands of times. The company has called surprise billing a “source of contracting negotiating leverage” to demand higher payments from insurers.
“Underneath this are patients who may well be charged outrageous amounts of money, but that’s just not a core consideration,” said Joshua Sharfstein, a professor of health policy and management at the Johns Hopkins Bloomberg School of Public Health. “The situation a lot of patients feel like they’re in is they’re collateral in this financial tug of war.”
TeamHealth and Envision Healthcare have poured millions into political ads attacking surprise billing legislation. The companies have said they want to settle out-of-network bills through arbitration instead of using average local rates, as some lawmakers have proposed.
As an alternative to going after patients themselves, TeamHealth said it sues insurers to demand higher payments for out-of-network charges. The company has filed 38 such lawsuits since 2018.
In the Texas case, two TeamHealth affiliates that provide doctors and nurses to emergency rooms in the Houston and El Paso areas sued a small insurance company called Molina Healthcare. TeamHealth identified almost 5,000 out-of-network claims in 2016 and 2017 for which it billed $6.6 million and Molina paid $760,000. TeamHealth sent a letter demanding that Molina pay $2.3 million. Molina’s lawyers viewed this as an admission that the original bill was far higher than even TeamHealth thought was fair.
The actual costs of medical services are not a factor in setting TeamHealth’s prices, according to the deposition of Kent Bristow, a TeamHealth executive in charge of revenue. At some locations, TeamHealth’s prices were higher than those of 95% of other providers and eight or nine times more than what Medicare would pay, according to Bristow’s deposition.
Most of the two TeamHealth affiliates’ charges were never actually collected, according to their tax returns and a deposition of the accountant who prepared them. For the years 2016 and 2017, the two affiliates billed a combined $1.9 billion, the tax returns show. But $1.1 billion, or 58%, was discounted according to negotiated deals with insurers. An additional $528 million was written off as bad debt that would never get repaid. So the combined revenue that the two affiliates actually received across the two years was $274.5 million, or about 14% of the amount initially billed, according to the tax returns.
The amount that TeamHealth charges doesn’t determine how much TeamHealth pays its doctors who perform those services, the company’s chief financial officer, David Jones, said in an October 2019 deposition. Instead, the doctors are paid a base compensation plus an incentive tied to how much work they do (which is not the same as the price billed for their services). For the two TeamHealth affiliates in the Molina case in 2016 and 2017, the company paid doctors a total of $170.5 million, or 62% of the net revenue, according to the tax returns. Other health care providers such as nurse practitioners and scribes received another $48.4 million.
The administrative services that TeamHealth provides — such as billing, printing and malpractice insurance — added up to $29.5 million, according to the tax returns.
After covering all those expenses, the amount of money left over — commonly called profit — was $26.1 million, about 10% of the two affiliates’ net revenue in 2016 and 2017. (The accounting method that TeamHealth uses for its tax returns is different from how it prepares financial statements regulated by the Securities and Exchange Commission. Under the latter method, the tax returns note a total of $36.8 million for the two affiliates in 2016 and 2017. Because of these accounting variations, it’s impossible to compare the figures on the TeamHealth affiliates’ tax returns to profits reported by publicly traded health care companies.)
The TeamHealth executive in charge of the two affiliates said he assumed the profit would be shared with the doctors who did the work. “It would most likely go back to the providers,” the executive, Lance Williams, said in a deposition. Under further questioning, he admitted, “Yeah, I’m not sure.”
In fact, the entire leftover $26.1 million went to TeamHealth’s “management fee.” The management fee is not a fixed rate but rather everything that remains after covering costs, regardless of the amount, according to the CFO’s deposition. “If the revenues exceed the expenses, that is essentially the management fee,” Jones said.
In other words, out of the $1.6 billion that was originally billed but not collected, any additional dollar that TeamHealth managed to recover would be passed through to the corporate parent. The doctors would not see it.
Jones said doctors benefit from increasing collections because their incentive-based pay is adjusted over time. In addition, Bristow said the management fee is not the same as profit because there may be additional expenses at the corporate level.
“The economic benefits created by these practices, any profit, if you will, ultimately flows up to the TeamHealth entity,” Ron Luke, a health economics expert hired by Molina, said in a deposition.
To establish this business model, TeamHealth had to find a way to deal with long-standing state laws that were specifically designed to protect the medical profession from becoming beholden to profit motives. These laws, known as the corporate practice of medicine doctrine, require doctors to work for themselves or other doctors, not lay people or corporations like TeamHealth. Court records in the Molina case show how TeamHealth’s lawyers use shell entities to avoid directly employing doctors.
“TeamHealth monetizes this process by unilaterally setting charges and then billing patients and payors for those amounts and retaining all of the profits of the enterprise,” Robert McNamara, a former president of the American Academy of Emergency Medicine, wrote in a memo as an expert witness against TeamHealth in the lawsuit. “The fees generated, billed, and retained by TeamHealth reflect the type of overt commercialization of the medical profession that the prohibition on the [corporate practice of medicine] is designed to prevent.”
TeamHealth said its business arrangements comply with all laws and no court or agency has ever found otherwise. “TeamHealth’s clinicians are supported by a world-class operating team that provides them with comprehensive practice management services that allow our clinicians to focus on the practice of medicine,” the company said. Envision Healthcare also said it follows all local, state and federal laws and regulations.
State laws against the corporate practice of medicine date as far back as the 19th century, as doctors strove to distinguish themselves from quacks and snake oil salesmen. According to the American Medical Association, the laws are meant to prevent profit motives from influencing medical judgments — a recognition that corporations’ devotion to shareholder value shouldn’t mix with doctors’ Hippocratic oath.
Another way to think about it is: Practicing medicine requires a license, and only a real human being can possibly have the education, training and character qualifications that licensing boards require.
Courts have scrutinized these arrangements for decades. No judge has ever ruled that TeamHealth or Envision Healthcare specifically violate state licensing rules. But such allegations have repeatedly cropped up in lawsuits involving the companies, some of which settled favorably to the other side, according to McNamara, who was consulted on many of the cases.
TeamHealth and Envision have themselves acknowledged that they operate on questionable legal ground. During periods when the companies were publicly traded, their investor disclosures highlighted the controversy surrounding their compliance with state licensing regimes. TeamHealth and Envision said they believed their business models were legal but recognized that prosecutors, regulators and judges could conclude otherwise. TeamHealth specifically cited “laws prohibiting general business corporations, such as us, from practicing medicine.”
“While we believe that our operations and arrangements comply substantially with existing applicable laws relating to the corporate practice of medicine and fee splitting, we cannot assure you that our existing contractual arrangements, including restrictive covenant agreements with physicians, professional corporations and hospitals, will not be successfully challenged in certain states as unenforceable or as constituting the unlicensed practice of medicine or prohibited fee splitting,” the company said in its 2015 annual report. “In this event, we could be subject to adverse judicial or administrative interpretations or to civil or criminal penalties, our contracts could be found to be legally invalid and unenforceable or we could be required to restructure our contractual arrangements with our affiliated provider groups.”
TeamHealth says the laws are outdated and unnecessary — as one of the company’s senior lawyers called it in a deposition, “this arcane law we call the corporate practice of medicine that nobody needs.”
Not all states have such laws. In Florida, for instance, TeamHealth employs doctors directly. In states that have laws against the corporate practice of medicine, TeamHealth has a workaround depending on the specific requirements in that state. Here’s how it works for the affiliates involved in the Molina litigation, just two out of hundreds of equivalent arrangements around the country.
Doctors working for TeamHealth are technically independent contractors to a “professional association,” or P.A. In order to comply with Texas law, the professional association is owned by a licensed physician. The professional association then contracts with TeamHealth subsidiaries to provide administrative services — such as billing, payroll and malpractice insurance — in exchange for payment.
These professional associations, however, are hardly independent. They’re “owned” by an executive at TeamHealth, and the company has the power to remove and replace him at any time. For the two professional associations involved in the Molina case, when a new executive took over as “owner” in 2019, he said in a deposition that he couldn’t remember how he “bought” the entities or if he ever paid anyone the $2 nominal price of their shares.
“Everything about your right to own, operate, and manage ACS and EST [the two professional associations] is dependent upon you staying in the good graces of the TeamHealth organization, correct?” Molina’s lawyer asked in the deposition.
“Correct,” the owner/executive, Lance Williams, said.
“And if you were fired for any reason, you would lose ownership of ACS and EST, lose the right to manage ACS and EST, correct?”
“Correct.”
Williams also said there’s no “black and white” separation between clinical and financial issues.
In sum, the contract between TeamHealth and the professional associations gives investors more control of the business than doctors, according to Chuck Pine, a financial investigator who specializes in examining shell companies to determine the real beneficial owners. Pine isn’t involved in the Molina litigation.
Molina’s lawyers called the arrangement “a sham to permit TeamHealth to unlawfully practice medicine by allowing it to in effect employ physicians in violation of state law.”
TeamHealth countered that whether or not Molina’s claims are right, they aren’t enforceable through private litigation; only the state’s attorney general could prosecute a corporation for practicing medicine without a license.
The judge rejected Molina’s claims in an order that didn’t explain her rationale. Other parts of the case are still pending.
TeamHealth has used the same argument to defeat other lawsuits. It puts opponents in a Catch-22: State licensing boards have no control over a corporation that might be practicing medicine without a license because the boards don’t license corporations. The boards could theoretically punish the “owners” of the professional associations, but those doctors are not always licensed in the same state as the practice, and TeamHealth could always replace them with someone else.
The Texas attorney general’s office didn’t respond to requests for comment. McNamara said he’s brought several cases to the attention of various state attorneys general, to no avail.

WASHINGTON – Cities were already grappling with the health and economic impact of COVID-19 when protests uncovered what one mayor Thursday called the “second pandemic” – a fractured police relationship with minority communities.
The comments came in a virtual roundtable discussion with mayors from across the country, including Phoenix Mayor Kate Gallego, who were asked to talk about “national unrest amid COVID-19 pandemic.”
Gallego was joined by mayors of Atlanta, Stockton, California, and Newark, New Jersey, who split the hour-long conversation evenly between cops and the coronavirus. While the discussion was wide-ranging, the mayors agreed on one thing: It’s a challenging time.
“It has been quite a few two weeks in Phoenix, Arizona,” Gallego said during the event, which was sponsored by the Center for American Progress. “We have been having robust conversations with the police department and our community.”
Cities across the country were rocked in recent weeks by protests over George Floyd’s May 25 killing at the hands of Minneapolis police officers, one of whom knelt one Floyd’s neck for almost 9 minutes despite pleas that he could not breathe.
A number of those protests erupted into clashes with police, with some protesters taking up “defund the police” as a rallying cry.